Hidden Artery Disease: Can New Blood Pressure Tests Better Predict Patient Survival?
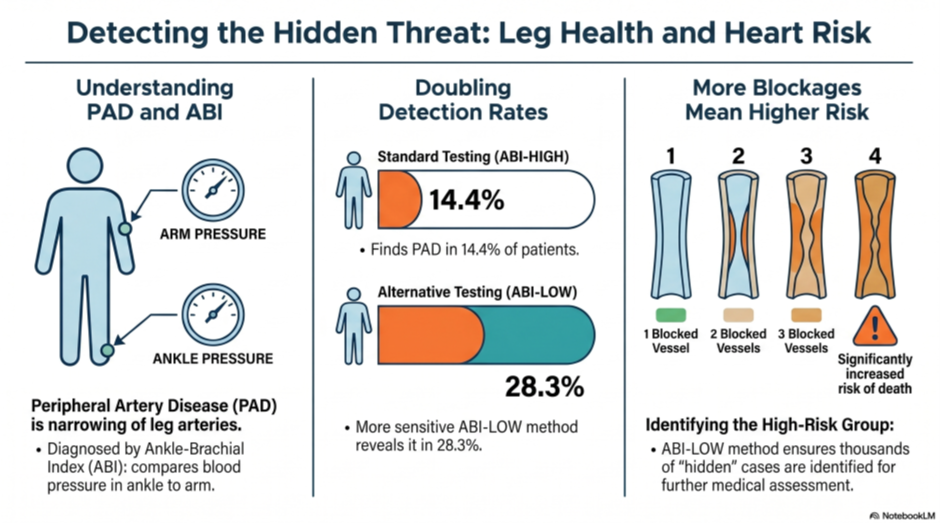
People with high blood pressure are at great risk for narrowed leg arteries, but the standard test—comparing blood pressure in the ankle to the arm—often misses early signs of the disease.
Researchers tracked nearly 22,000 patients with high blood pressure for five years to see if calculating the test differently (using the lowest blood pressure reading from the ankle instead of the highest) could better predict their chances of survival.
The new testing method found twice as many people with narrowed arteries (28.3%) compared to the standard method (14.4%), and confirmed that having more affected blood vessels significantly increases the risk of death.
While the new method is great at finding hidden cases, it only slightly improved the mathematical ability to predict long-term survival; however, it remains highly useful for doctors to identify patients who need closer monitoring.
Keywords
high blood pressure, narrowed arteries, blood pressure test, survival prediction, screening test
Further details
Kolossváry, Endre, Tamás Ferenci, Zoltán Járai, and Katalin Farkas. “Alternative ankle–brachial assessments show no significant added value in predicting mortality of hypertensive patients.” Journal of Hypertension 44, no. 4 (2026): 682-690.
Abstract
Background: Peripheral artery disease (PAD), assessed via the ankle–brachial index (ABI), is a recognized form of hypertension-mediated organ damage (HMOD). While alternative ABI calculations have shown improved sensitivity for PAD detection, their prognostic utility in hypertensive populations remains unclear. Methods: In this prospective cohort study of 21875 hypertensive individuals (ERV Study), we compared the prognostic performance of three ABI-based approaches: standard ABI using the higher ankle pressure (ABI-HIGH), ABI using the lower ankle pressure (ABI-LOW), and multivessel ABI scoring (number of vessels with ABI <= 0.90). The primary endpoint was all-cause mortality, assessed over a median follow-up of 5years using interval-censored Cox regression. Results: PAD prevalence was 14.4% using ABI-HIGH and 28.3% using ABI-LOW, with 13.9% of patients identified only by the latter. All PAD definitions were independently associated with mortality. ABI-LOW as a continuous variable demonstrated the strongest association (hazard ratio 1.87; 95% CI, 1.63–2.16). Multivessel ABI showed a dose–response relationship with mortality. However, overall discrimination was modest: time-dependent AUCs ranged from 0.608 to 0.635 for ABI-based models alone. When added to clinical predictors, ABI metrics improved the AUC to a range from 0.763 to 0.780, with added predictive value between 6 and 11%. Conclusion: In hypertensive individuals, ABI-LOW and multivessel scoring identify more PAD cases and are independently associated with mortality. However, their incremental value in mortality risk prediction is limited. Alternative ABI methods may assist in identifying higher risk subgroups warranting further vascular assessment.
Keywords
ankle–brachial index, hypertension, mortality prediction, peripheral artery disease
The original publication can be accessed at the following link: https://doi.org/10.1097/HJH.0000000000004255